Anterior Lumbar Interbody Fusion (ALIF)
In any spinal fusion, two or more vertebrae are fixed in position and stabilized after a degenerated disc is removed so they become, essentially, a single unit. They are held in position using hardware — a “cage” and screws — that prevents them from moving independently and causing pain. Traditionally, a neurosurgeon would make an incision in the patient’s back to reach the vertebrae that need to be fused. In an anterior lumbar interbody fusion (ALIF) procedure, the neurosurgeon makes the incision on the front (anterior) side of the patient.
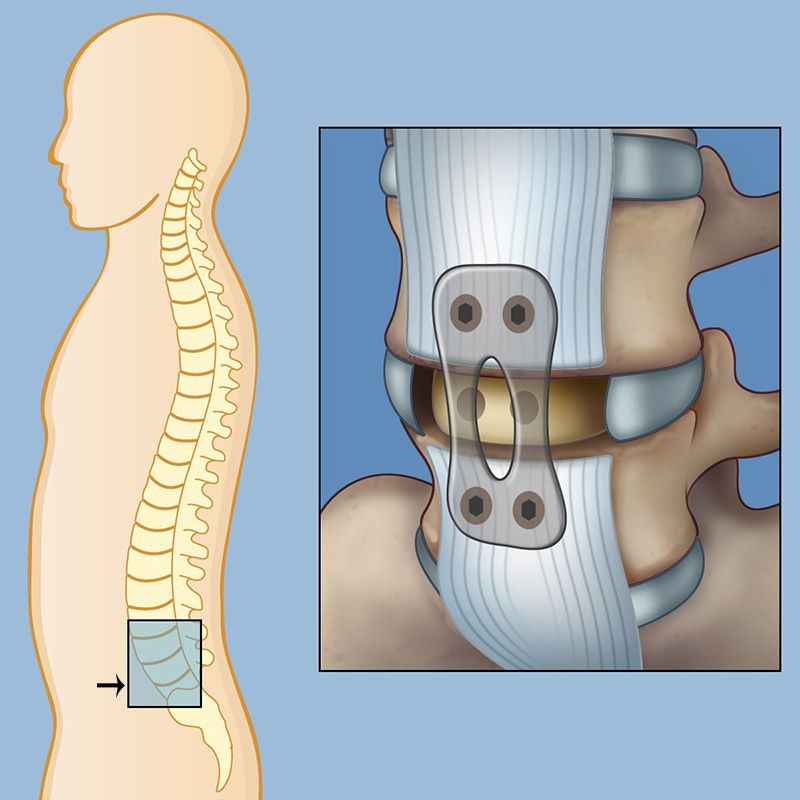
The anterior approach allows a neurosurgeon to insert a larger cage than possible with the traditional posterior (back) approach. The larger cage creates a better curvature to the lower (lumbar) spine, where it is needed for stability and posture. Our spinal surgery experts work alongside specially trained vascular surgeons during the ALIF procedure to safely navigate around the blood vessels in front of the spine.
In some severe cases, the neurosurgeon uses a posterior approach in addition to the anterior fusion to provide the most optimal stability. Not everyone is a good candidate for ALIF. Neurosurgeons identify which patients are candidates for ALIF as opposed to a traditional posterior approach based on a careful physical exam and detailed review of imaging tests.
MI-TLIF Spine Fusion
Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) is an advanced minimally invasive procedure for spinal fusion, in which vertebrae are stabilized to take pressure off nerves and relieve back pain. It is a minimally invasive alternative to older, more invasive methods of spinal fusion, which were more painful and required longer recovery periods. TLIF is performed through two very small incisions in the back, so patients experience less pain, shorter recovery times, and fewer surgical complications.
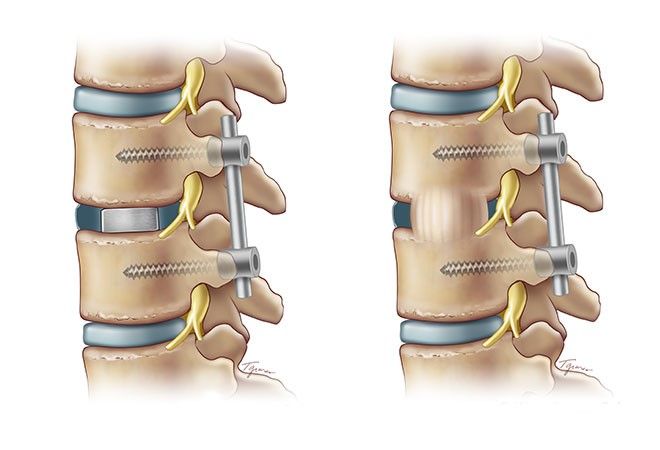
Spinal fusion procedure, the neurosurgeon inserts a "cage" between the affected vertebrae (left) to restore proper positioning. Six to twelve weeks later (right) bone graft material hardens over the cage, making the fusion permanent.
LLIF (Lateral Lumbar Interbody Fusion)
Lateral lumbar interbody fusion, more commonly referred to as LLIF, is an advanced minimally invasive spine procedure that approaches from the side, avoiding the major muscles of the back. LLIF is a general term for lateral approaches to the spine. Other acronyms that refer to minor alterations on this procedure are DLIF (direct lateral interbody fusion), XLIF (extreme lateral interbody fusion), OLIF (oblique lumbar interbody fusion), and ATP (anterior-to-psoas). A spine surgeon makes a small incision in the patient’s side between the lower ribs and pelvis, then inserts a special surgical instrument just above the disc space. The surgeon removes the damaged disc tissue and inserts a spacer between the vertebrae. The surgical team monitors the position and correct placement of the spacer, sometimes using special screws or a plate on the side of the spine to offer additional stability. Patients typically are walking within a few hours of the LLIF procedure and are then discharged the next day.
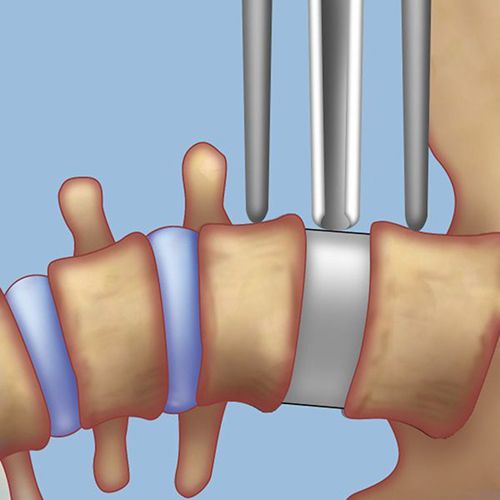
In the LLIF procedure, a neurosurgeon approaches the spine from the side and inserts a spacer to correct curvature.






Reviewed by: Osama Kashlan, MD, MPH
Last reviewed/last updated: November 2024
Illustrations by Thom Graves, CMI
