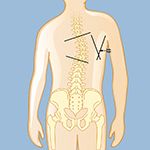
The degree of curvature is measured by drawing lines at the first and last tilted vertebrae, then drawing lines perpendicular to those lines. Where that second set of lines intersect, called the Cobb angle, is where the degree of the curve is measured.
Scoliosis can be classified in many ways. One of the most common ways to classify scoliosis is by severity of the curve. Mild scoliosis is when the curve is between 10 to 25 degrees. Moderate is when the curve is between 26 and 45 degrees. Severe scoliosis occurs when the curve is greater than 45 degrees.
Scoliosis can often be clearly visible especially when it is moderate or severe. However, to establish the extent of a scoliosis and its cause, a neurosurgeon or orthopedic physician will begin by getting a complete medical history, including viewing any prior X-rays. The physician will look for asymmetries (uneven appearances) as a person sits, stands, and walks, paying special attention to the shoulders, ribs, chest, leg length, and other unusual findings, such as if the torso doesn’t appear to be evenly positioned over the pelvis, or a person’s head seems off-center. Current physical findings and measurements will be compared to prior records.
Other information will be gathered as well, including:
Scoliosis can be visualized with X-rays.
○ Front-view full-length X-rays of the spinal column are taken as the individual stands while keeping the head erect
○ Lateral-bending X-rays may be taken from the side while an individual is standing or bending sideways or backwards to determine flexibility of the curve
Other tests may be ordered to diagnosis adult scoliosis and determine its severity and cause.










Reviewed by: Osama Kashlan, MD, MPH
Last reviewed/last updated: November 2024
Illustrations by Thom Graves, CMI
